Knee Arthroscopic Surgery
Anatomy of the Knee
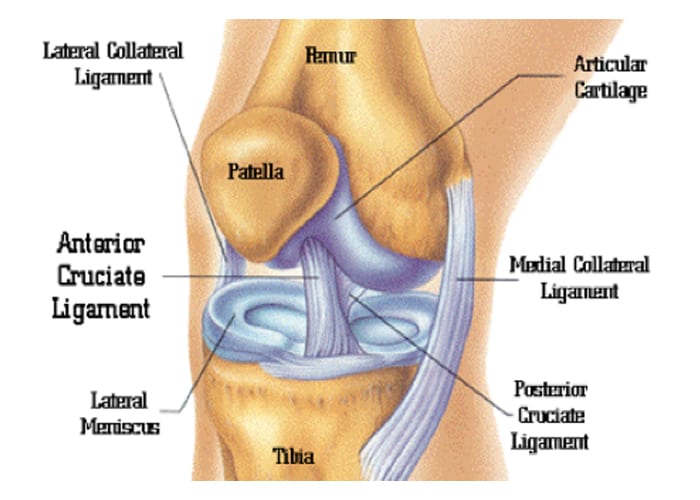
The knee joint is made up of the femur (thigh bone), tibia (lower leg bone), and patella (knee cap). All these bones are lined with articular cartilage. This articular cartilage acts like a shock absorber and allows a smooth, low friction surface for the knee that allows it to move. Between the femur and tibia lie the medial meniscus and the lateral meniscus. The menisci are stabilizers and act as shock absorbers by dispersing the weight of the body and reducing friction during movement. The knee is also stabilized by ligaments that are both inside and outside the joint. The medial and lateral collateral ligaments support the knee from excessive side to side movement. The (internal) anterior and posterior cruciate ligaments support the knee from buckling and giving way. The knee joint is surrounded by a capsule that produces a small amount of synovial (lubricating) fluid to help with smooth motion. The plica is an extension of the protective synovial capsule of the knee. The plica tissue is located along the medial side of the knee.
Knee Arthroscopy
This is a minimally invasive surgical procedure in which an examination and treatment of a joint is performed using an arthroscope. During the arthroscopy, the surgeon examines and repairs your injured or diseased joint with the help of an optical instrument called an arthroscope. An arthroscope is a thin fiber-optic scope which is about the diameter of a drinking straw. It is fitted with a miniature camera and light source. Other tools used are shavers, lasers, and a type of biting tool.
Procedures
Conditions treated with arthroscopic surgery of the knee include: torn meniscus, torn anterior cruciate ligament (ACL), inflamed or damaged lining of the joint, misalignment of the kneecap/patella, bone spurs or loose bodies, arthritis, and scarring or tissue inflammation within joints.
Indications: An arthroscopy may help if you have persistent pain, catching, or swelling in your knee, and you have tried conservative treatment, such as Physical Therapy and anti-inflammatories, an arthroscopy may help.
Anesthesia: General anesthesia is used unless contraindicated. You will receive certain medications through your IV that make you unconscious and unable to feel pain during your surgical procedure.
Surgery Time: In most arthroscopic surgeries of the knee it will take approximately 15-20 minutes. ACL repair can take 30-60 minutes.
Hospital Stay: You will be in the hospital approximately 5 hours. This is an outpatient procedure and rarely do you have to stay overnight.
Average Total Recovery Time: Total recovery time is from 2-4 weeks for a simple arthroscopy, and from 6 to 8 weeks for an ACL repair.
Procedures:
- Meniscectomy is the surgical removal of part of a torn or frayed meniscus. The torn portion or unstable meniscal fragments are removed and the edges of the remaining meniscus are shaved to make the meniscus smooth.
- Anterior Cruciate Ligament (ACL) Reconstruction is a surgical tissue graft replacement of the ACL. The torn ligament is removed from the knee before the graft is inserted. The graft is usually an allograft, which is the tissue from a donor tissue. An autograft is an option which involves the medical grafting of tissue from the patient’s body. The recovery time for this procedure is 6-8 weeks. You will start wearing a range of motion brace the day of surgery and you will wear this for approximately 4-6 weeks. It will be locked at full extension until you see you see Dr. Bramlett or a therapist and it should be worn at all times. It is important for you to see Dr. Bramlett in the office 2-4 days after surgery and will then be instructed on exercises and possible physical therapy.
- Plica resection is the surgical resection of the inner lining of the knee joint. The plica irritates and rubs the distal femoral condyle. This tissue can be resected during arthroscopy.
- Lateral release is a surgical procedure to release tight capsular structures, for example, the lateral retinaculum on the outer aspect of the kneecap. This is usually performed due to the kneecap is being pulled over to the outer side of the knee and is not tracking properly in the groove of the femur bone as the knee bends and straightens.
- Debridement is the cleaning out of the knee joint and the smoothing of the surfaces of the joint.
Incision: Two ½ inch incisions underneath the patella with one or two stitches each. Sometimes these stitches are subcuticular and will dissolve over time. You will have the two stitches underneath the patella for an ACL repair, and a 2-inch incision on the anterior proximal tibia which will be closed with staples.
Possible Complications: Complications include infection, nerve damage, circulatory damage, and an anesthesia risk.
Before being discharged:
- Make sure you void before leaving the hospital.
- Make sure your drain is removed before being discharged
Normal Post-Operative Occurrences: You will experience swelling, redness, pain or discomfort, bruising of the lower leg, and blood-tinged drainage. This is normal. You may also have an elevated temperature just from having surgery; this can be treated with Tylenol. If your temperature stays above 101⁰ and is not brought down with Tylenol, please let us know. Ice your knee every hour for 20 minutes for the pain and swelling.
Dressing: For the first 48 hours you will have a large, soft dressing, which starts 10-12 inches above the knee and extends to your ankle. Please wear something large to the hospital which will go over this bandage when it is time to be discharged home.
Shower: A shower is permitted after removing the bandages 48 hours after your surgery. Rinse incisions, but do not rub or use soap. Clean your incisions with alcohol after getting out of the shower and apply bandaids. It helps the swelling when you wrap your knee with an ace wrap for several days after removing bandages.
Medications: Your prescriptions will consist of two types of pain medications, usually Percocet or Norco. Phenergan may also be given for nausea, if needed. You may resume your anti-inflammatory medicine following surgery. If you do not take any, you may take Advil/Ibuprofen, or Aleve with a Tylenol for swelling and pain control. Pain medication can cause constipation, so increase the bulk in your diet and take a laxative if needed. Over-the-counter medications are less likely to cause this problem.
Pain: You will experience some degree of pain after surgery. Pain and swelling may increase based on your activity level, so be sure to elevate and ice when this occurs.
Icing After Surgery
We highly recommend a Game Ready ice machine for icing your knee. It is a machine with a sleeve that covers your knee from mid-thigh to mid-calf and is connected to a hose and a reservoir that holds ice and water. Instead of using ice from the freezer, you can freeze 14- 8-oz bottles of water. Use 7 of them in the Game Ready reservoir at a time. It helps with pain, bruising, and swelling. We highly recommend you rent a Game Ready since physical therapy is not required. Reserve a Game Ready before your surgery by calling the representative for Game Ready, Kameron, at 205-269-0200. Insurance does not cover it and your cost is $100 a week.
Activity: You may need crutches or a walker for a couple of days after surgery until you are able to walk without assistance. For the first two days you should take it easy. Elevate your leg on 3-4 pillows above the heart, and use ice 20-30 minutes every hour for swelling and pain. While in recovery you may start exercising doing quad isometric exercises. You can begin riding a stationary bicycle 3-4 days after surgery or walking on level ground. Remember to start out slow and increase your exercising gradually. Always ice after exercising.
Exercises
Remember to ice your knee after exercising.
- Quad isometric exercises:
Extend your leg and flex your foot toward your face. Tighten your quads. Hold for 20 seconds. Repeat 10 times. Do this 3-4 times a day.
- Pumping your feet:
Pump your feet throughout the day. This helps with blood flow.
- Recumbent bike:
Ride a recumbent bike starting 3-4 days after surgery. Start out riding the bike 10 minutes, increase your time gradually, until you are riding the bike 20-30 minutes. Remember,
ONLY ride it every other day.
- Knee Flexion/Extension Exercises:
Lean back in chair or lie down on bed. Raise operative leg up and grasp your thigh with both hands, slowly straighten leg, and let knee bend letting gravity pull foot down. Do this 3-4 times slowly, three or four times a day.
Returning to Work:
- You should be able to resume desk work and light duty activity in 3 to 7 days, and more strenuous activity in 2 weeks.
- Job duties will dictate return to work.
- If excessive walking is required and light duty cannot be arranged, you should be able to return to work in 2 weeks.
- If a great deal of climbing and lifting is required, you may need to be off work 3-4 weeks.
Return to Office: Your post-op appointment will need to be 7-14 days after surgery. Please call (205) 783-5900 to make that appointment.
Our team has developed this treatment guide in order for you to have a quick reference for your care and recovery. We have made a very simple protocol to enable you an easier recovery. It is my pleasure to be able to diagnose and treat my patients, and we will do whatever is necessary to assist you with your recovery and satisfaction.